Research and Development Interests
Historically, my interests revolve around these economic, finance, managerial accounting and health care policy, management and administration concentrations, among others:
Constitutional Political Economy: My review of constitutional political economy in the tradition of F.A. Hayek and James Buchanan with a particular emphasis on constitutional culture. For example, how do we empower the state [hospitals, doctors, nurses, and clinics] to do good things, while preventing it from taking our lives and property because of medical debt? What about EMTALA? Is it even possible? What institutions actually promote and help humans to thrive, etc?
Institutional Economics: My study of the economic impact of various rules about financial institutions and financial regulations (HIPAA, Dodd-Frank, ACA and Sarbanes Oxley in healthcare), monetary institutions and central banks, the Euro, business firm, venture capital, entrepreneurship and corporate culture, etc.
Austrian Economics: My thinking on Ayn Rand with special interest in the “the use of knowledge in society problem”; the epistemic foundations of limited government; and any thinking on social networks, philosophy and politics. I also research Austrian economic insights on central banking, business cycle theory and economic methodology; as well as the sociology, psychology and risky behavioral considerations of investment management and economics.
And, to evaluate health care economics and finance in the United States, I reviewed three categories of data that together created a comprehensive view of the overall quality of health care. These categories include:
- Health outcomes, including indicators such as rates of disease and risk factors like obesity and smoking, preventable deaths and infant mortality. These measures help answer the question: How healthy are the people who live here?
- Cost, including factors like how much the state spends on health care and the average cost of private health insurance. These measures help answer the question: How expensive is health care in a state, region or population?
- Access, including data on the number of primary care providers and hospital beds available, how many people are uninsured and how many people need care but have difficulty getting it. These indicators help answer the question: How easy is it to get the health care in a specific cohort?
But, most recently, I have been researching, crafting, developing and writing three [3] grant funded health economics, policy, management and social-psychology text books as a re-imagined and insightful linguistical free-market capitalistic trilogy to be released in 2024-25 [vox populi]. And, another work-in-progress on podiatric medical and surgical practice [vox podiatry].
***
THREE HEALTH ECONOMICS TEXT BOOKS CURRENTLY IN-PROGRESS [Major Grant-Funded and Working Research & Development Publications-in-Process]

1. PARADOXICAL HEALTH ECONOMICS [A Treatise Torching Absurd Myths and Self-Contradictory Ethical Propositions]
The term “paradox” signifies a contradiction of some sort. Modern health care appears to be rich in contradictions, and it is claimed to be paradoxical in a number of ways. In particular health care is held to be a paradox itself: it is supposed to do good, but is accused of doing harm. The objective of this book is to investigate whether the concept of paradox can serve as a framework for analyzing pressing problems in modern health care economics. To pursue this, three distinctive levels of paradox are identified: resolvable paradoxes, anti-nomies and aporias. The analysis reveals that when facing the challenges of modern health economics, the focus of attention should be to resolve the resolvable ethical paradoxes, to acknowledge the anti-nomies and to learn to live with the aporias.
So, what are the most important health economic paradoxes of the last century? We have some ideas and that’s the question we attempt to ask, ponder and explain in this treatise? And, although, there is a natural overlap with the fields of finance and accounting; there is little emerging specificity and no prioritized importance to this alphabetized ranking.
Inevitably some good paradoxical theories fell by the wayside during curation, often for reasons unrelated to their importance. And, the line between theory and concept gets blurry at times. So, please take the alphabetized list in the spirit of curiosity mixed with seriousness. And, keep in mind, that important health economic paradoxes are not always permanently correct. So, mixed among the most important paradoxical theories you may find a few that are wrong, or inexact, despite their influence. See if you can find them. We could go on, but you get the idea.
Moreover, as we will illustrates, there are nuances about what constitutes a paradoxical theory — some try to describe how the concept works, and others try to describe how it should work. And, of course, they vary widely in how well they accomplish those goals. And, as the list may suggest, we undoubtedly overlooked some worthy or less orthodox theories. (And we probably overlooked some mainstream items, too!).
For example: Cosmetic surgery is becoming increasingly popular worldwide. The “cosmetic surgery paradox” describes the phenomenon whereby women are both encouraged to undergo cosmetic surgery and condemned for doing so. Cosmetic surgery advertisements, media, and government policy all contribute to the rise in cosmetic surgery.
For example: The male-female health-survival paradox, also known as the morbidity-mortality paradox or gender paradox, is the phenomenon in which women experience more medical conditions and disability during their lives, but they unexpectedly live longer than men.
For example: For decades, US taxpayers have been lamenting the high cost of health care. Since the mid-1980s, Americans have had double-digit spending on health care. Despite this investment, Americans are less healthy than their European and Scandinavian counterparts across an array of health measures.
***
2. HOBSON’S CHOICE MEDICINE [Exposing Crowd-Sourced Reflections on Ethical Decision-Making, Health Economics, Linguistics and Free Market Enterprise]
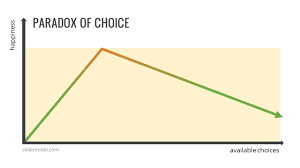
For those unfamiliar with this economics expression, it means …‘no choice at all’. Now, this is very different than transparent cognitive decision-making science that offers a real choice. In other words: this choice or that one –OR– the either / or fallacy whereby the arguer characterizes a complex problem with many possible solutions, as having only two outcomes. One outcome is desirable and one not. But, with a true Thomas Hobson’s choice dilemma; there is No real choice at all!
That’s where omy research is focused, and why this book is titled: HCM. In fact, I seek to illustrate the many false choices that all four participants in the US healthcare system quartet [patients – payers – providers – public policymakers] face … and often unwittingly make each day. For example:
Patients: “This health plan covers all drug costs” … As long as they are in our generic formulary.
Payers: “The government does not force anyone to buy health insurance” … The choice is to buy insurance or pay a higher tax bill [“fee” or “penalty”].
Providers: “You don’t have to sign an insurance Hold Harmless Contract Clause to indemnify us for a malpractice claim” … But, you may be de-selected from our health insurance panel if you don’t.
Public Policymakers: “You can keep your doctor” … As long as s/he is in our narrow PP-ACA insurance network of physicians, medical centers and hospitals.
***
3. HEALTH ECONOMIC FOR ALL OF US – VITAL EXPLANATIONS FOR THE REST OF US [A Compendium of Lay Terms We All Should Know]

What are the most important free-market and Keynesian health economic theories of the last century? I have some ideas and that’s the question we attempt to ask, ponder and explain in this book? And, although, there is a natural overlap with the fields of finance and accounting; there is little emerging specificity and no prioritized importance to this alphabetized ranking.
Now, this text is written for non-specialist and lay readers with little to no prior knowledge of health economics, finance, health insurance or related theories. While we use many named theories we use non-technical terms about the origin, structure, development and eventual contemporary use of them which is the objective for the study of modern health economics. I present information, in compendium form, about basic core concepts like theories, laws, rules, charts, eponyms and even oddities in a communicator fashion of subject mater expertise.
For example: A trained insurance professional who can help you enroll in a health insurance plan. Agents may work for a single health insurance company. You won’t pay anything additional if you enroll with an agent. Agents must be licensed in their states and have signed agreements to sell health plans. In many states, agents are not required to act in a consumer’s best interest. However:
- Agents often get payments (“commissions”) from insurance companies for selling plans. Some may not sell plans of companies they don’t represent.
- You may qualify for a premium tax credit and other savings if you enroll with an agent.
For example: In health insurance, diverse selection is a market situation where buyers and sellers have different information. The result is that participants with key information might participate selectively in trades at the expense of other parties who do not have the same information. But, adverse selection occurs when buyers and sellers of a health insurance product do not have the same information available. Also known as the “lemon problem” by economist George Akerlof 1970 who examined how the quality of goods traded in a market can degrade in the presence of information asymmetry between buyers and sellers, leaving only “lemons” behind.
- Nicotine: Someone with a nicotine dependency getting health insurance at the same rate of someone without nicotine dependency. Gross obesity, smoking, STDs, drug abuse, and automotive speed racing may be similar situations.
- Time lag: When a person waits until s/he knows s/he is sick and in need of health care before applying for a health insurance policy.
Research & Development: marcinko-research-statement-pdf
***
TRUE TALES FROM THE FOOT EXAM ROOM:[Bizarre Patient Encounters from a Podiatrist]. Personal and bizarre patient office and hospital encounters over a career of more than two decades. Some are morbid, some are sad and others are hysterical. All are presented in a witty and fascinating fashion.

Content copyrighted 2000-2027 and to present. All rights reserved. USA.
 As a former academic Scholar and Dean, appointed and Endowed Department Chair, Distinguished Professor and physician-executive, David Edward Marcinko MBBS DPM FACFAS MBA MEd BSc CMP® is originally from Loyola University MD, Temple University in Philadelphia and the Milton S. Hershey Medical Center in PA; Oglethorpe University, Emory University and Atlanta Hospital & Medical Center in GA; the Kellogg-Keller Graduate School of Business and Management in Chicago; and Aachen City University Hospital, Koln-Germany. He is one of the most innovative global thought leaders in medical, financial, economics and business management and didactic entrepreneurship education today by leveraging and adding value with strategies to grow revenues and EBITDA while reducing nonessential expenditures and improving operational efficiencies. Dr. Marcinko is a board certified physician, surgical fellow, hospital medical staff Vice President, public and population health advocate, and Chief Executive & Education Officer with more than 400 published papers; 5,150 op-ed pieces and over 135+ domestic / international presentations to his credit; including the top 10 biggest pharmaceutical companies and financial services firms in the nation. He is also a best-selling Amazon author with 30 published text books in four languages [National Institute of Health, Library of Congress and Library of Medicine]. Dr. Marcinko is past Editor-in-Chief of the prestigious "Journal of Health Care Finance", and a former Certified Financial Planner®, who was named "Health Economist of the Year" in 2010, by PM magazine. He is a Federal and State court approved expert witness featured in hundreds of peer reviewed medical, business, management and trade publications [AMA, ADA, APMA, AAOS, Physicians Practice, Investment Advisor, Physician's Money Digest and MD News]. As a licensed insurance agent, RIA and SEC registered endowment fund manager, Dr. Marcinko is Founding Dean of the fiduciary focused CERTIFIED MEDICAL PLANNER® chartered designation education program; as well as Chief Editor of the HEALTH DICTIONARY SERIES® Wiki Project. His professional memberships include: ASHE, AHIMA, ACHE, ACME, ACPE, MGMA, FMMA and HIMSS. Dr. Marcinko is a MSFT Beta tester, Google Scholar, "H" Index favorite and one of LinkedIn's "Top Cited Voices". Presently, Professor Marcinko is "ex-officio" and R&D Scholar-on-Sabbatical for iMBA, Inc.
As a former academic Scholar and Dean, appointed and Endowed Department Chair, Distinguished Professor and physician-executive, David Edward Marcinko MBBS DPM FACFAS MBA MEd BSc CMP® is originally from Loyola University MD, Temple University in Philadelphia and the Milton S. Hershey Medical Center in PA; Oglethorpe University, Emory University and Atlanta Hospital & Medical Center in GA; the Kellogg-Keller Graduate School of Business and Management in Chicago; and Aachen City University Hospital, Koln-Germany. He is one of the most innovative global thought leaders in medical, financial, economics and business management and didactic entrepreneurship education today by leveraging and adding value with strategies to grow revenues and EBITDA while reducing nonessential expenditures and improving operational efficiencies. Dr. Marcinko is a board certified physician, surgical fellow, hospital medical staff Vice President, public and population health advocate, and Chief Executive & Education Officer with more than 400 published papers; 5,150 op-ed pieces and over 135+ domestic / international presentations to his credit; including the top 10 biggest pharmaceutical companies and financial services firms in the nation. He is also a best-selling Amazon author with 30 published text books in four languages [National Institute of Health, Library of Congress and Library of Medicine]. Dr. Marcinko is past Editor-in-Chief of the prestigious "Journal of Health Care Finance", and a former Certified Financial Planner®, who was named "Health Economist of the Year" in 2010, by PM magazine. He is a Federal and State court approved expert witness featured in hundreds of peer reviewed medical, business, management and trade publications [AMA, ADA, APMA, AAOS, Physicians Practice, Investment Advisor, Physician's Money Digest and MD News]. As a licensed insurance agent, RIA and SEC registered endowment fund manager, Dr. Marcinko is Founding Dean of the fiduciary focused CERTIFIED MEDICAL PLANNER® chartered designation education program; as well as Chief Editor of the HEALTH DICTIONARY SERIES® Wiki Project. His professional memberships include: ASHE, AHIMA, ACHE, ACME, ACPE, MGMA, FMMA and HIMSS. Dr. Marcinko is a MSFT Beta tester, Google Scholar, "H" Index favorite and one of LinkedIn's "Top Cited Voices". Presently, Professor Marcinko is "ex-officio" and R&D Scholar-on-Sabbatical for iMBA, Inc.








![Financial Management for Healthcare Organizations [Two-Volume Journal]](https://i0.wp.com/davidedwardmarcinko.com/wp-content/uploads/2016/07/untitled1.png?w=209&h=209&crop=1&ssl=1 "Financial Management for Healthcare Organizations [Two-Volume Journal]")

![Financial Planning for Physicians [From Leading CMPs®]](https://i0.wp.com/davidedwardmarcinko.com/wp-content/uploads/2016/06/51gilfji5wl1.jpg?w=209&h=209&crop=1&ssl=1 "Financial Planning for Physicians [From Leading CMPs®]")